GBM remains the most common and aggressive malignancy of the central nervous system,2 accounting for approximately 80% of all malignant primary brain tumours.3 Despite medical advances, the prognosis of GBM remains poor and the recurrence rate is still high due to its highly invasive nature.4 Current standard of care includes maximal safe resection followed by radiotherapy (RT) and chemotherapy (temozolomide [TMZ]).3 The randomized phase III EORTC-NCIC study showed that at the 5-year follow-up, the median overall survival of patients with GBM who received concomitant and adjuvant TMZ and RT was 14.6 months.5
The therapeutic value of TTFields was explored initially in human glioma cell lines (U-118 and U-87).6 In vitro results showed that the optimal TTFields frequency was 200kHz, similar to that observed in rat glioma cell lines.6 In vivo studies confirmed in vitro findings and demonstrated that the application of 200 kHz TTFields at 2 V/cm for six days resulted in a reduction in tumour size in rats compared with control.6 These outcomes subsequently led to testing TTFields in clinical studies, including the phase III studies which were designed to investigate the efficacy and safety profile of TTFields in patients with newly diagnosed GBM7 and recurrent GBM.8
References:
- U.S. Food and Drug Administration approval. Available at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P100034S013. Accessed 6 April 2022.
- Davis ME, et al. Clin J Oncol Nurs. 2016;20:S2–S8.
- Hanif F, et al. Asian Pac J Cancer Prev. 2017;18:3–9.
- Burri SH, et al. Am J Clin Oncol. 2018;41:191–196.
- Stupp R, et al. Lancet Oncol. 2009;10:459–466.
- Kirson ED, et al. Proc Natl Acad Sci USA. 2007;104:10152–10157.
- Stupp R, et al. JAMA. 2017;318:2306–2316.
- Stupp R, et al. Eur J Cancer. 2012;48:2192–2202.
EF-14 study in newly diagnosed GBM
EF-14 study was a multicentre, open-label, randomized clinical phase III study which recruited 695 patients with newly diagnosed GBM from 83 sites in North America, Europe, Korea and Israel.2 The objective of the study was to investigate the efficacy and safety of TTFields, when used in combination with TMZ in this patient group.2
Study design 2
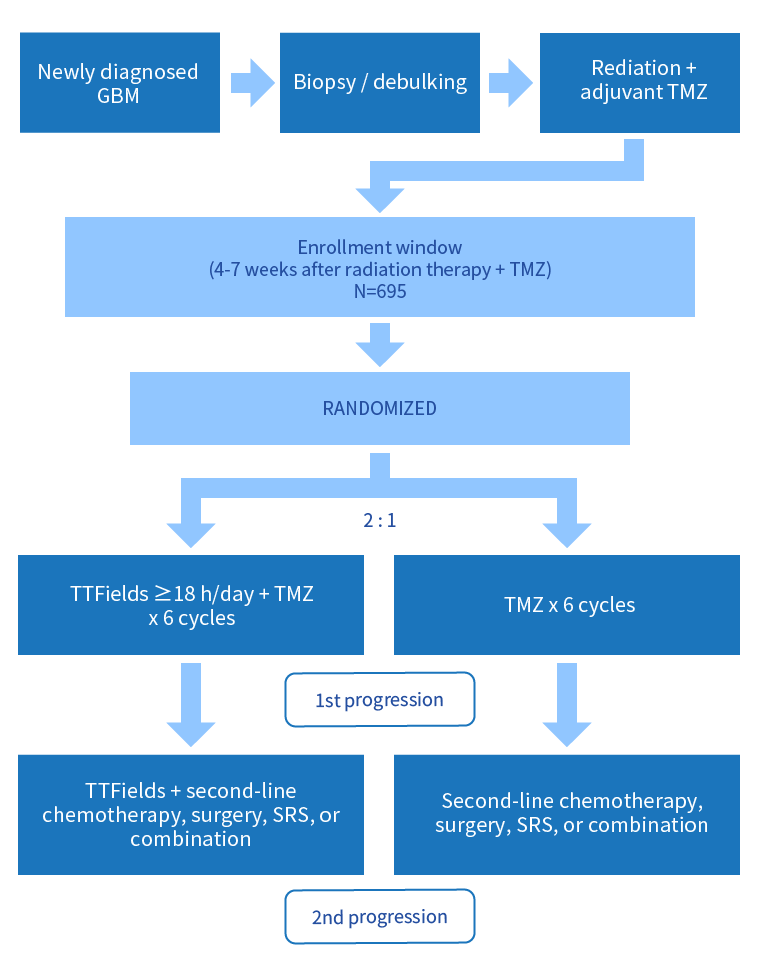
GBM, glioblastoma multiforme; SRS, stereotactic radiosurgery, TMZ, temozolomide
- Primary endpoint: Progression-free survival (PFS)
- Secondary endpoint: Overall survival (OS)
- Exploratory endpoints: Rate of PFS at 6 months, safety, health-related quality of life (HRQoL)
The study recruited patients with newly diagnosed GBM who completed radiation therapy and adjuvant TMZ.2 Patients were randomized at a 2:1 ratio to receive either TMZ (150–200 mg/m2/d for 5 days every 28 days for six cycles) with or without the addition of TTFields applied at a frequency of 200 kHz to the scalp.2 While patients in the control arm received second-line therapy based on best local practice if second progression was observed, those in the experimental arm continued to receive TTFields until second radiologic progression or for a maximum of 24 months.2
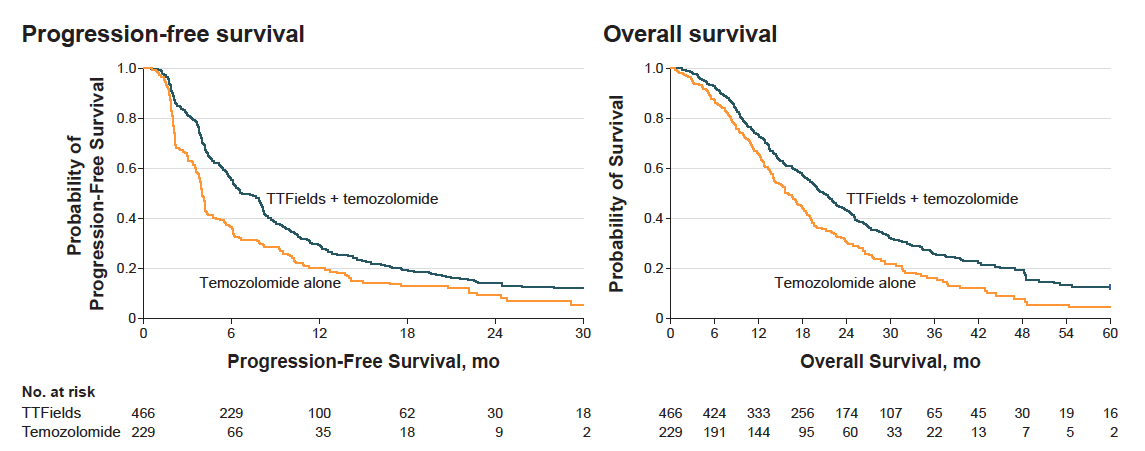
Efficacy – 5-year survival analysis
The 5-year survival analysis results from the intent-to-treat population are summarized below2:
| TMZ + TTFields (n=466) | TMZ only (n=229) | |
|---|---|---|
| Median PFS | 6.7 months | 4.0 months |
| (HR 0.63; 95% CI, 0.52–0.76; p<0.001) | ||
| Median OS | 20.9 months | 16.0 months |
| (HR 0.63; 95% CI, 0.53–0.76; p<0.001) | ||
The median follow-up time was 40 months. CI, confidence interval; HR, hazard ratio; OS, overall survival; PFS, progression-free survival; TMZ, temozolomide
The annual survival rates have been indicated below, demonstrating that survival benefits of those receiving TTFields and TMZ persisted with prolonged treatment2:
| TTFields + Temozolomide (n=466) | Temozolomide Alone (n=229) | Between-Group Differences | |
|---|---|---|---|
| Annual survival rates (%) | |||
| Year 1 | 73 (69-77) | 65 (59-72) | 8 (0-16) |
| Year 2 | 43 (39-48) | 31 (25-38) | 12 (4-18) |
| Year 3 | 26 (22-31) | 16 (12-23) | 10 (3-17) |
| Year 4 | 20 (16-25) | 8 (4-14) | 12 (5-19) |
| Year 5 | 13 (9-18) | 5 (2-11) | 8 (2-14) |
Post hoc analysis showed that the increased OS was consistent across all subgroups which favoured the use of TTFields and TMZ 2:
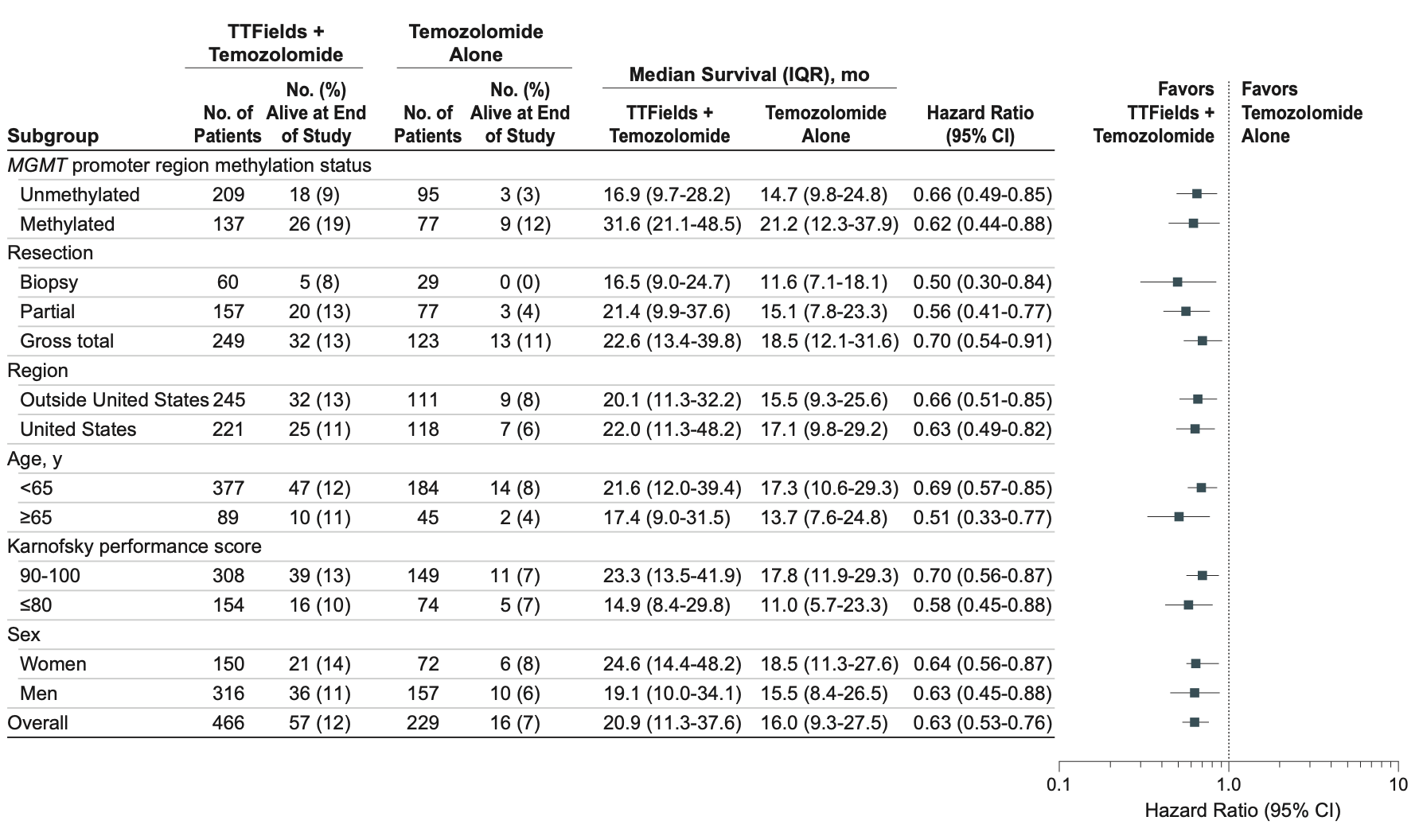
CI, confidence interval; IQR, interquartile range
Safety
Safety data showed that the addition of TTFields to chemotherapy was not associated with any significant increase in the rates of systemic adverse events compared with TMZ alone (48% vs 44%, respectively; p=0.58).2 However, more patients receiving TTFields and TMZ experienced localised skin toxicity compared with those who received TMZ alone, contributed by medical device site reaction beneath the transducer arrays.2 Amongst those who were treated with both TTFields and TMZ, a majority of patients (52%) had mild to moderate skin irritation and 2% of patients had severe (grade 3) skin irritation.2 However, overall incidence, distribution and severity of adverse events were also comparable in both groups.2
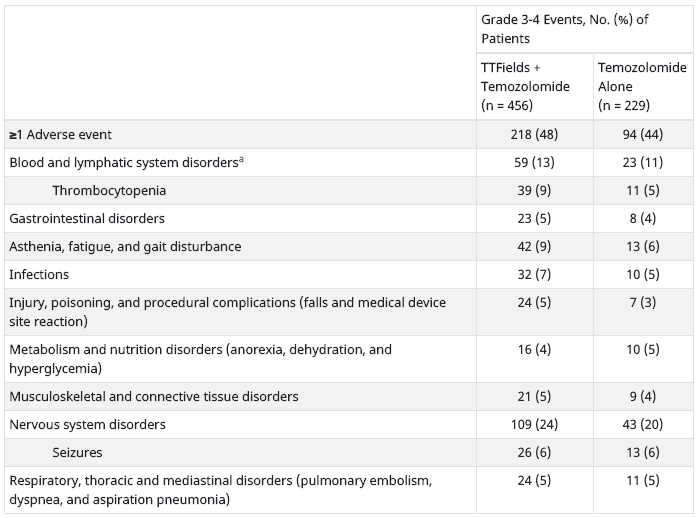
| Grade 3-4 Events, No. (%) of Patients | ||
|---|---|---|
| TTFields + Temozolomide (n = 456) |
Temozolomide Alone (n = 229) |
|
| ≥1 Adverse event | 218 (48) | 94 (44) |
| Blood and lymphatic system disordersa | 59 (13) | 23 (11) |
| Thrombocytopenia | 39 (9) | 11 (5) |
| Gastrointestinal disorders | 23 (5) | 8 (4) |
| Asthenia, fatigue, and gait disturbance | 42 (9) | 13 (6) |
| Infections | 32 (7) | 10 (5) |
| Injury, poisoning, and procedural complications (falls and medical device site reaction) | 24 (5) | 7 (3) |
| Metabolism and nutrition disorders (anorexia, dehydration, and hyperglycemia) | 16 (4) | 10 (5) |
| Musculoskeletal and connective tissue disorders | 21 (5) | 9 (4) |
| Nervous system disorders | 109 (24) | 43 (20) |
| Seizures | 26 (6) | 13 (6) |
| Respiratory, thoracic and mediastinal disorders (pulmonary embolism, dyspnea, and aspiration pneumonia) | 24 (5) | 11 (5) |
TTFields, tumor-treating fields. aThe numerically slightly higher incidence of haematological toxicity, fatigue, and some other adverse effects are due to the longer treatment duration and observation time in the experimental group. The differences disappear when data are normalized for treatment duration.
Compliance
Post hoc analysis of the EF-14 study showed that, in the TTFields plus TMZ group, patients who were treated with TTFields for ≥18 hours a day (monthly average in the first 6 months of treatment) had longer survival than patients treated <18 hours a day (22.6 months, 95% CI, 19.7-25.1 months vs 19.1 months, 95% CI, 16.5-21.9; HR, 0.65; 95% CI, 0.49-0.85; p=0.009).2
A forest plot depicting the relationship between TTFields compliance and survival benefits showed that in patients receiving both TTFields and TMZ that achieved 50% or more compliance had longer PFS and OS compared with those receiving TMZ alone. Furthermore, a progressive increase in survival benefits as compliance improved was observed in these patients.3
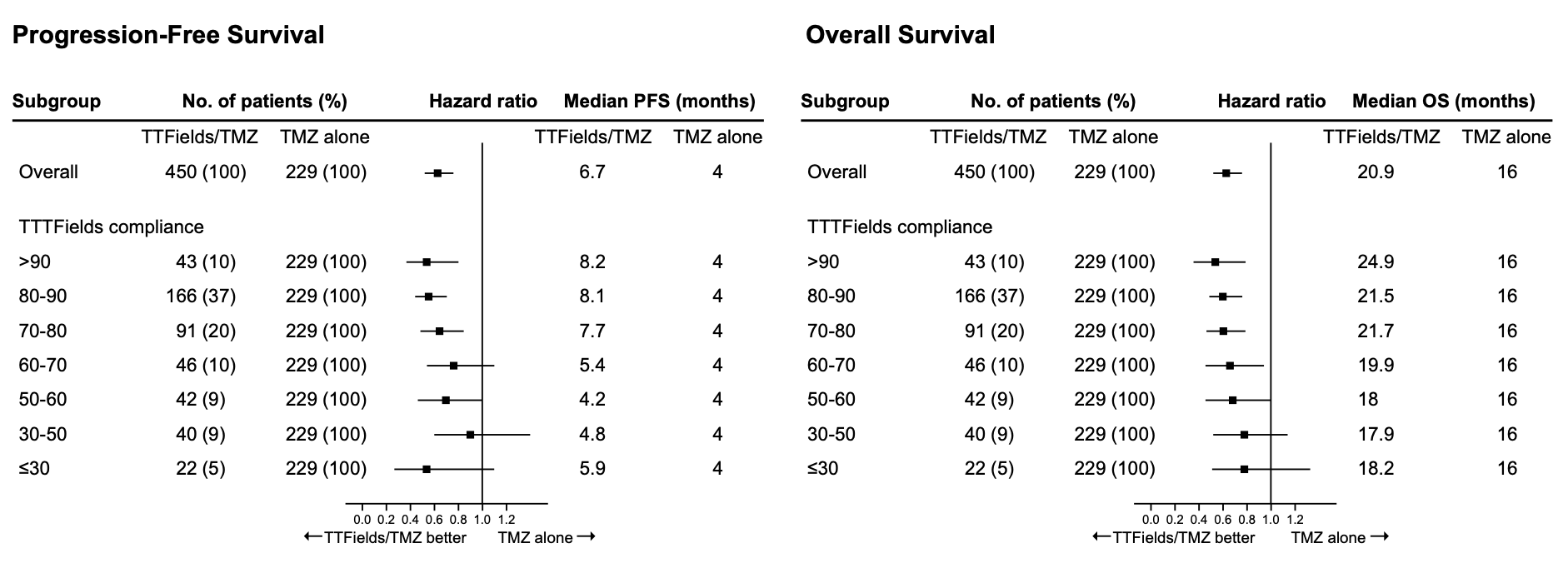
Patients with monthly compliance of more than 90%, in particular, had maximum survival benefits,3 suggesting the benefits associated with regular and prolonged use of TTFields in this patient group.3
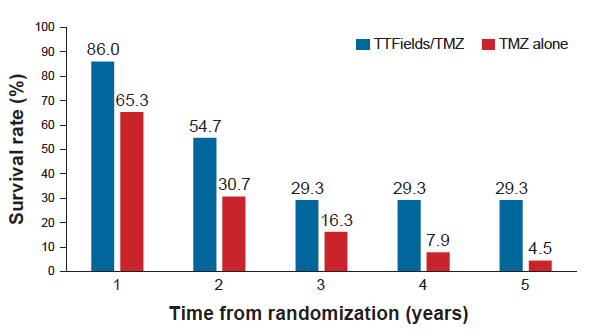
The annual survival rate in newly diagnosed GBM patients with compliance rates >90%. TTFields, tumor-treating fields; TMZ, temozolomide
Health-related quality of life (HRQoL)
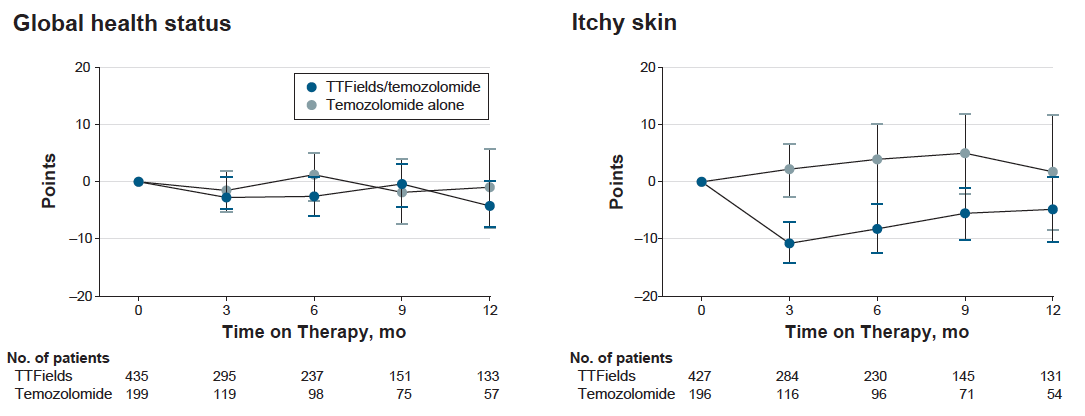
The evaluation of HRQoL was performed using the validated European Organisation for Research and Treatment of Cancer (EORTC) quality-of-life questionnaire (QLQ-C30) and brain module (QLQ-BN20).4 Nine predefined items were selected based on their relevance and the hypothesized effect of TTFields on HRQoL in patients with GBM.4 Raw scores were translated into a linear scale ranging from 0 to 100; a higher score represents a higher level of functioning.4 Difference of a minimum of 10 points was classified as a clinically meaningful change in any QoL scale. Patients were assessed for 12 months.
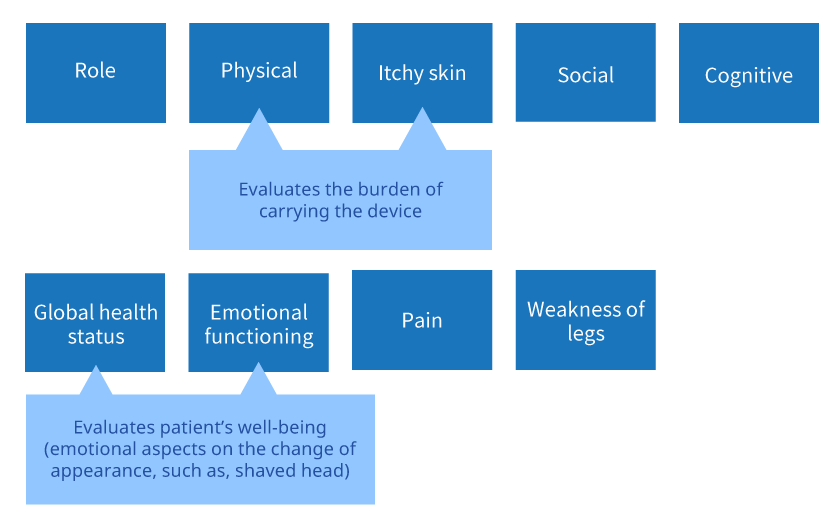
Results demonstrated that the addition of TTFields to standard treatment in patients who were also receiving TMZ did not have a negative impact on their HRQoL, except for itchy skin.4 Throughout the 12-month assessment period, mean changes from baseline were stable (<10-point change from baseline) for all nine predefined HRQoL scales in both arms with the exception of itchy skin.4 More patients receiving TTFields and TMZ showed improved or stable score for global health status compared with those receiving TMZ alone (53.5% vs 38.0%; p=0.001).4 Notably, more patients in the TTFields plus TMZ group showed significantly lower scores of itchy skin at 3, 6 and 9 months (all p<0.001), but not at 12 months, indicating that those patients initially experienced worse clinically relevant skin irritation compared with those receiving TMZ only.4
Furthermore, patients treated with TTFields and TMZ had a longer deterioration-free survival for global health, physical and emotional functioning, pain and weakness of legs compared with the chemotherapy arm.4 Time to deterioration was also measured and used as an indicator of the influence of treatment. Results showed that the score did not differ significantly except for itchy skin (favouring TMZ) and pain (favouring TTFields).4 Role, social, and physical functioning were not affected by TTFields.4
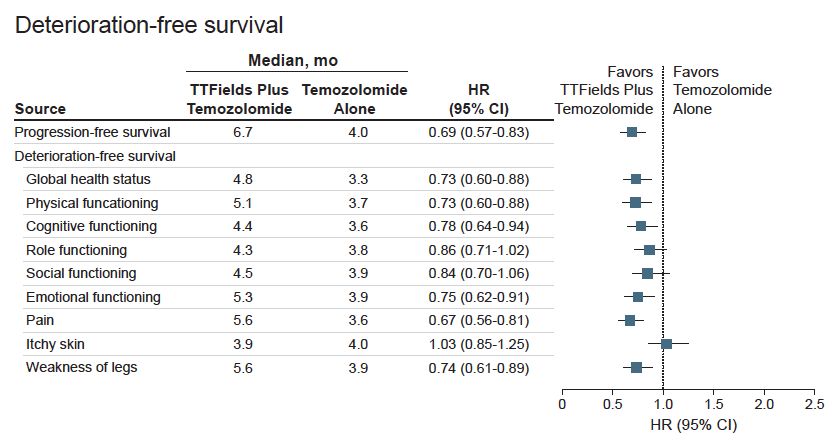
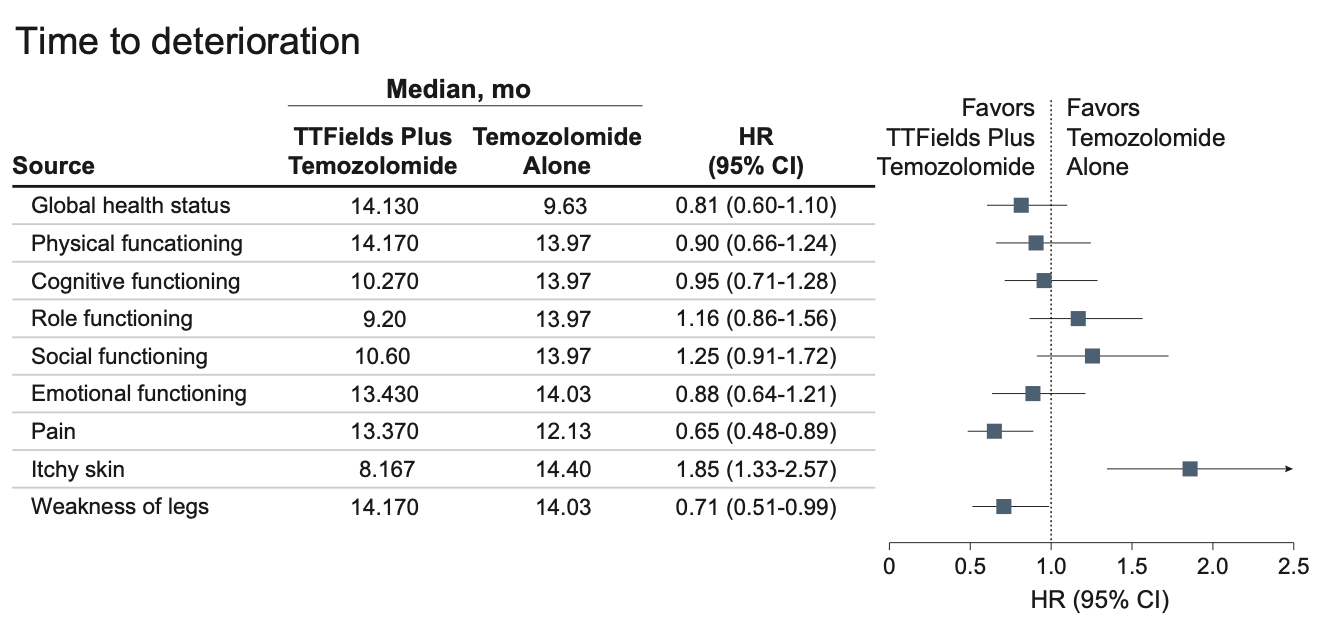
CI, confidence interval; HR, hazard ratio.
Post hoc analysis on continuation of TTFields with second-line treatment after first recurrence
After first recurrence, EF-14 patients were offered second-line treatment per local practice.2 However, in the TTFields plus TMZ arm, TTFields could be continued until second radiologic progression or for a maximum of 24 months.2 A post hoc analysis was conducted to evaluate the efficacy and safety of continuing TTFields with second-line treatment after first recurrence.5
Three hundred and ten patients in the original TTFields plus TMZ arm continued with TTFields and a further 26 patients in the TMZ alone arm crossed over to receive TTFields after first disease progression.5 One hundred and twelve patients in the TMZ alone arm received second-line treatment alone after progression.5
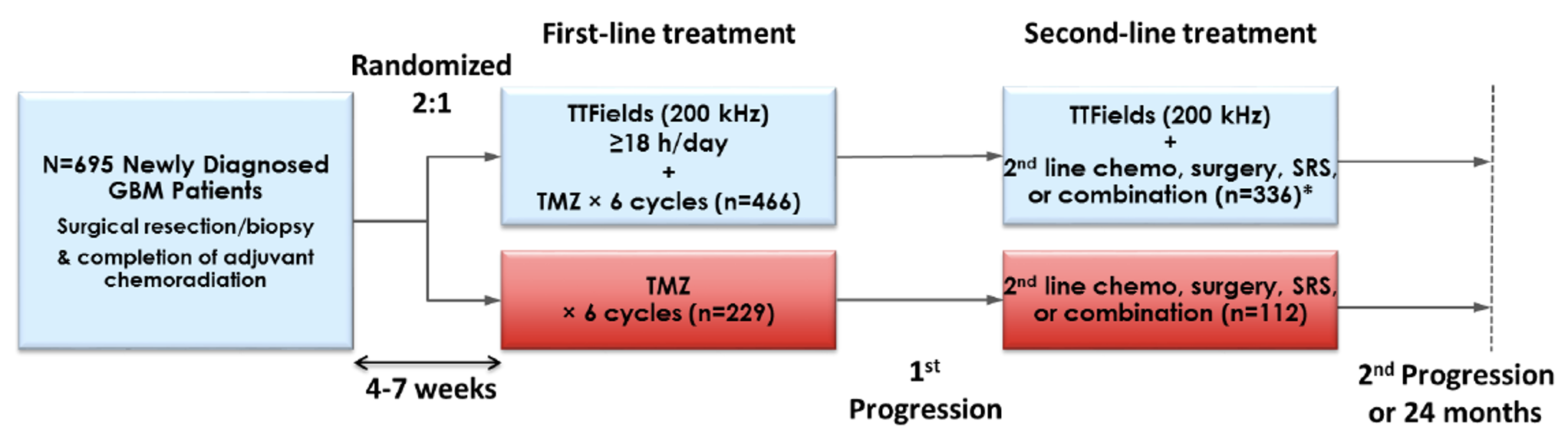
*Twenty-six TMZ alone patients crossed over to receive TTFields prior to second disease progression based on positive interim results. GBM, glioblastoma multiforme; SRS, stereotactic radiosurgery; TMZ, temozolomide; TTFields, tumor-treating fields. Adapted from Kesari S, et al. SNO Annual Meeting. 2017. Poster ACTR-55.
No significant differences were seen in second-line treatment between the two patient groups, with chemotherapy (55–84%) and bevacizumab (33–49%) being the most and second most frequent choices, respectively.5
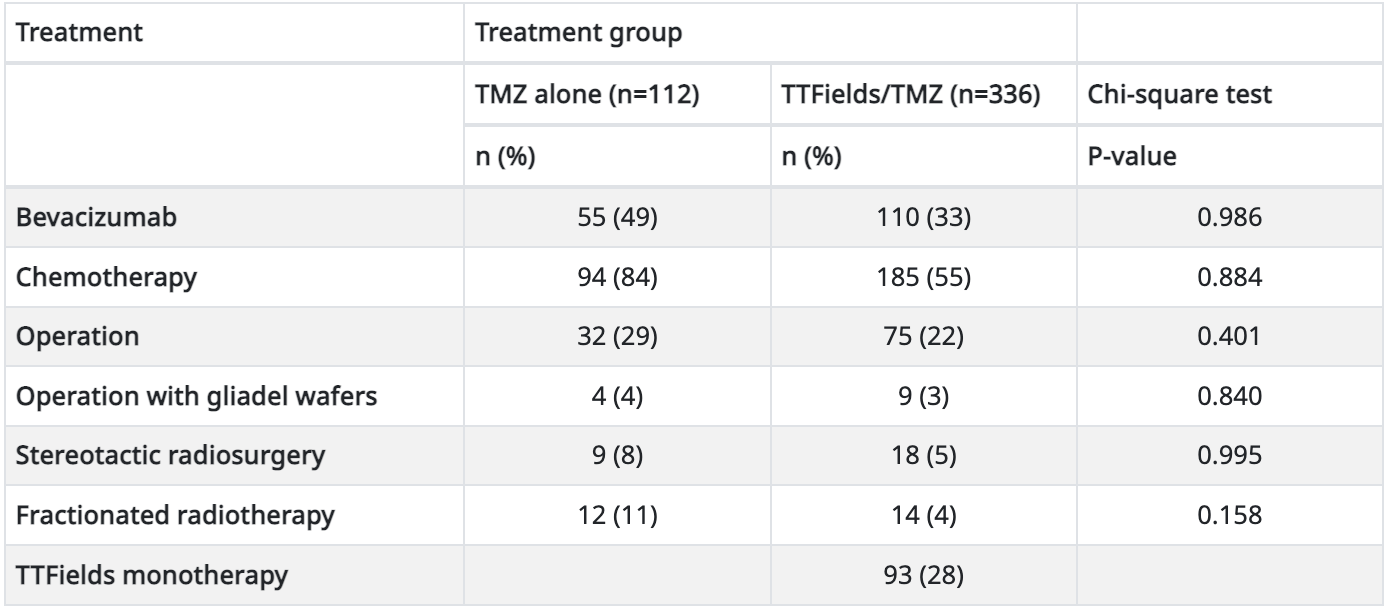
| Treatment | Treatment group | ||
|---|---|---|---|
| TMZ alone (n=112) | TTFields/TMZ (n=336) | Chi-square test | |
| n (%) | n (%) | P-value | |
| Bevacizumab | 55 (49) | 110 (33) | 0.986 |
| Chemotherapy | 94 (84) | 185 (55) | 0.884 |
| Operation | 32 (29) | 75 (22) | 0.401 |
| Operation with gliadel wafers | 4 (4) | 9 (3) | 0.840 |
| Stereotactic radiosurgery | 9 (8) | 18 (5) | 0.995 |
| Fractionated radiotherapy | 12 (11) | 14 (4) | 0.158 |
| TTFields monotherapy | 93 (28) | ||
TMZ, temozolomide; TTFields, tumor-treating fields.
Post hoc analysis showed that survival from the time of recurrence in patients receiving TTFields plus second-line treatment was significantly longer than that in patients receiving second-line treatment alone (12.0 months vs 10.8 months, respectively; HR: 0.75; 95% CI: 0.59–0.94; p=0.038).5
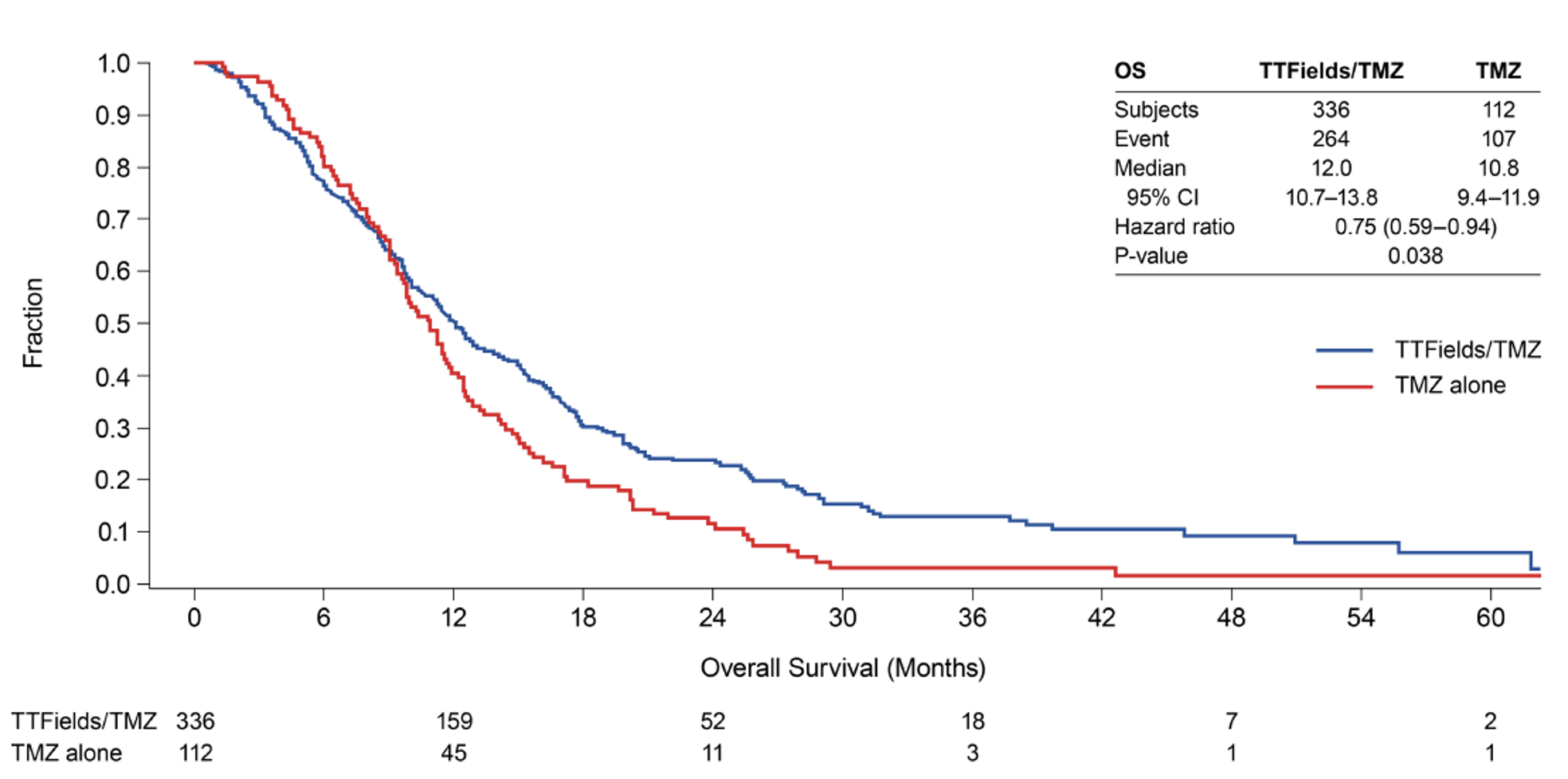
OS, overall survival from the time of recurrence; TMZ, temozolomide; TTFields, tumor-treating fields. Adapted from Kesari S, et al. SNO Annual Meeting. 2017. Poster ACTR-55.
Adverse events observed were consistent with those seen in the full study analysis and were similar between groups.5
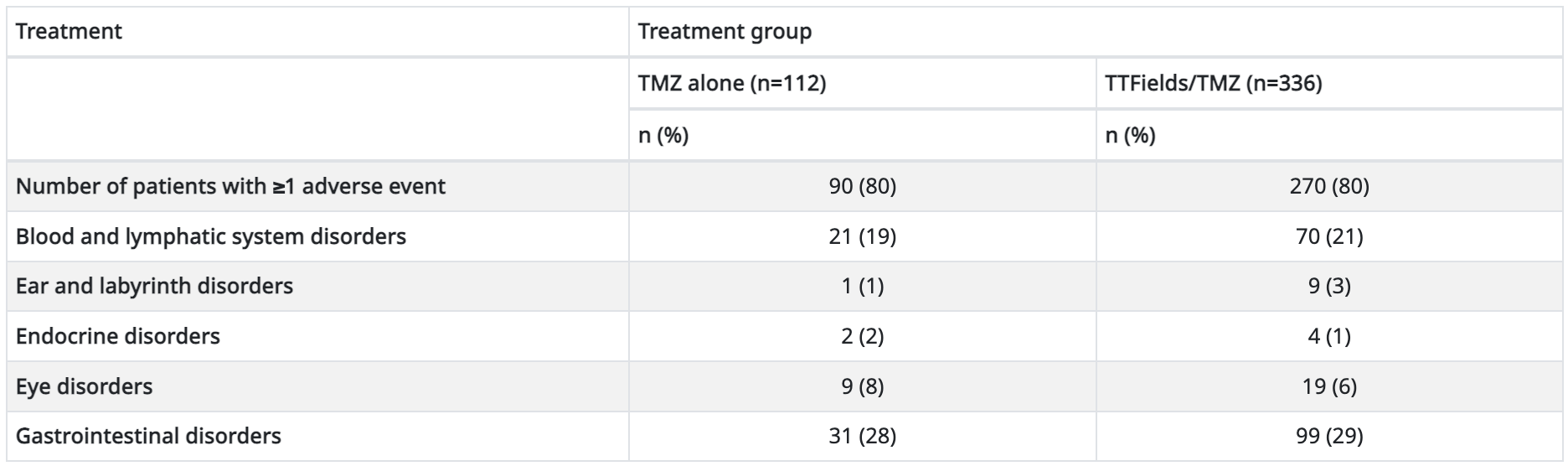
| Treatment | Treatment group | |
|---|---|---|
| TMZ alone (n=112) | TTFields/TMZ (n=336) | |
| n (%) | n (%) | |
| Number of patients with ≥1 adverse event | 90 (80) | 270 (80) |
| Blood and lymphatic system disorders | 21 (19) | 70 (21) |
| Ear and labyrinth disorders | 1 (1) | 9 (3) |
| Endocrine disorders | 2 (2) | 4 (1) |
| Eye disorders | 9 (8) | 19 (6) |
| Gastrointestinal disorders | 31 (28) | 99 (29) |
TMZ, temozolomide; TTFields, tumor-treating fields.
This post hoc analysis demonstrated that continuation of TTFields with second-line treatment after first tumor progression in patients with newly diagnosed GBM prolonged survival from the time of recurrence compared with TMZ followed by second line treatment alone.5
Korean subgroup analysis
Subgroup analysis of 39 Korean patients suggests that survival benefits were consistent with the intent-to-treat population of the EF-14 study.6 Korean patients who received combination treatment of TTFields and TMZ had significantly longer OS, as well as higher 1- and 2-year survival rates compared with those who received chemotherapy alone.6
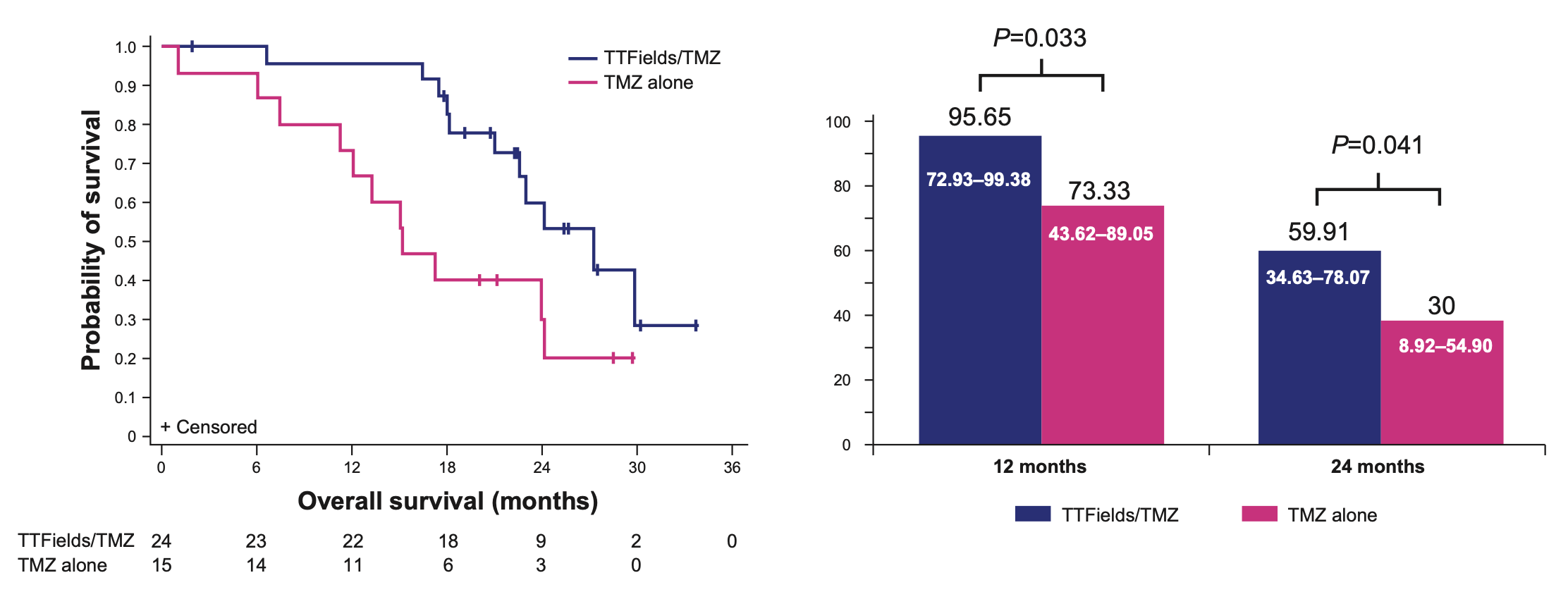
| TMZ + TTFields (n=24) | TMZ only (n=15) | |
|---|---|---|
| Median OS | 27.2 months | 15.2 months |
| (HR 0.27; 95% CI, 0.098–0.750; p=0.01) | ||
CI, confidence interval; HR, hazard ratio; OS, overall survival; TMZ, temozolomide
Subgroup analysis suggests that the prolonged OS observed in Korean patients may be associated with a longer mean duration of TTFields treatment compared with the entire EF-14 population (9.8 months vs 8.2 months).6 No significant difference between the incidence and type of adverse events was observed between the subgroup and the study population, however, numerically fewer Korean patients experienced skin irritation due to the prolonged use of TTFields through the transducer arrays compared with the intent-to-treat population (30% vs 44%).6
Elderly subgroup analysis
Elderly patients comprise a large segment of high-risk patients with GBM that are challenging to treat due to poor prognosis, frailty, comorbid conditions and increased risk of adverse events.7 The efficacy and safety of TTFields in elderly patients were evaluated in a subgroup analysis of EF-14 study.8
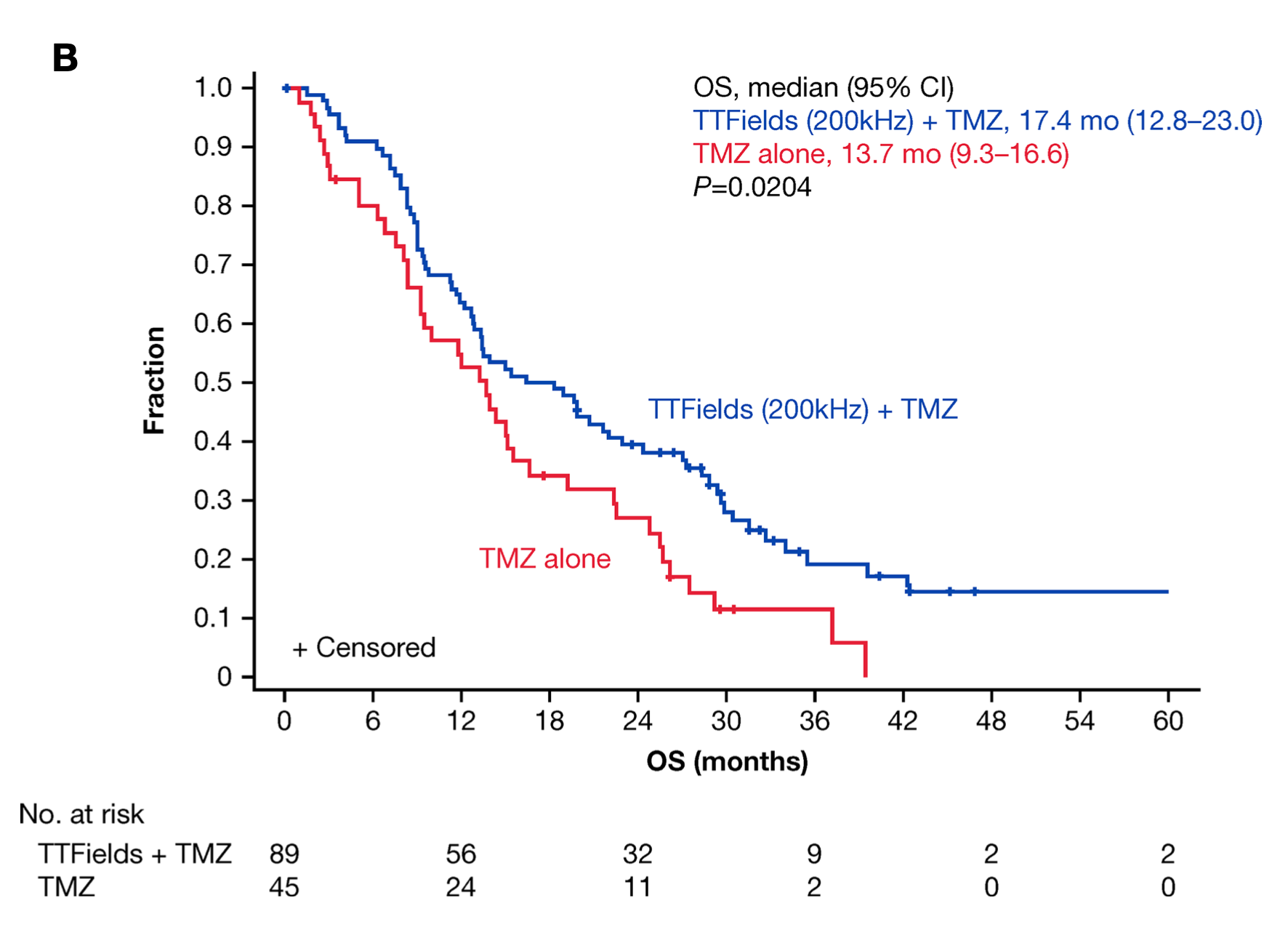
All 134 patients who were ≥65 years of age were included in this subgroup analysis (TTFields plus TMZ, n=89; TMZ alone, n=45).8 Significantly longer PFS and OS were observed in elderly patients treated with TTFields plus TMZ compared to those treated with TMZ alone.8
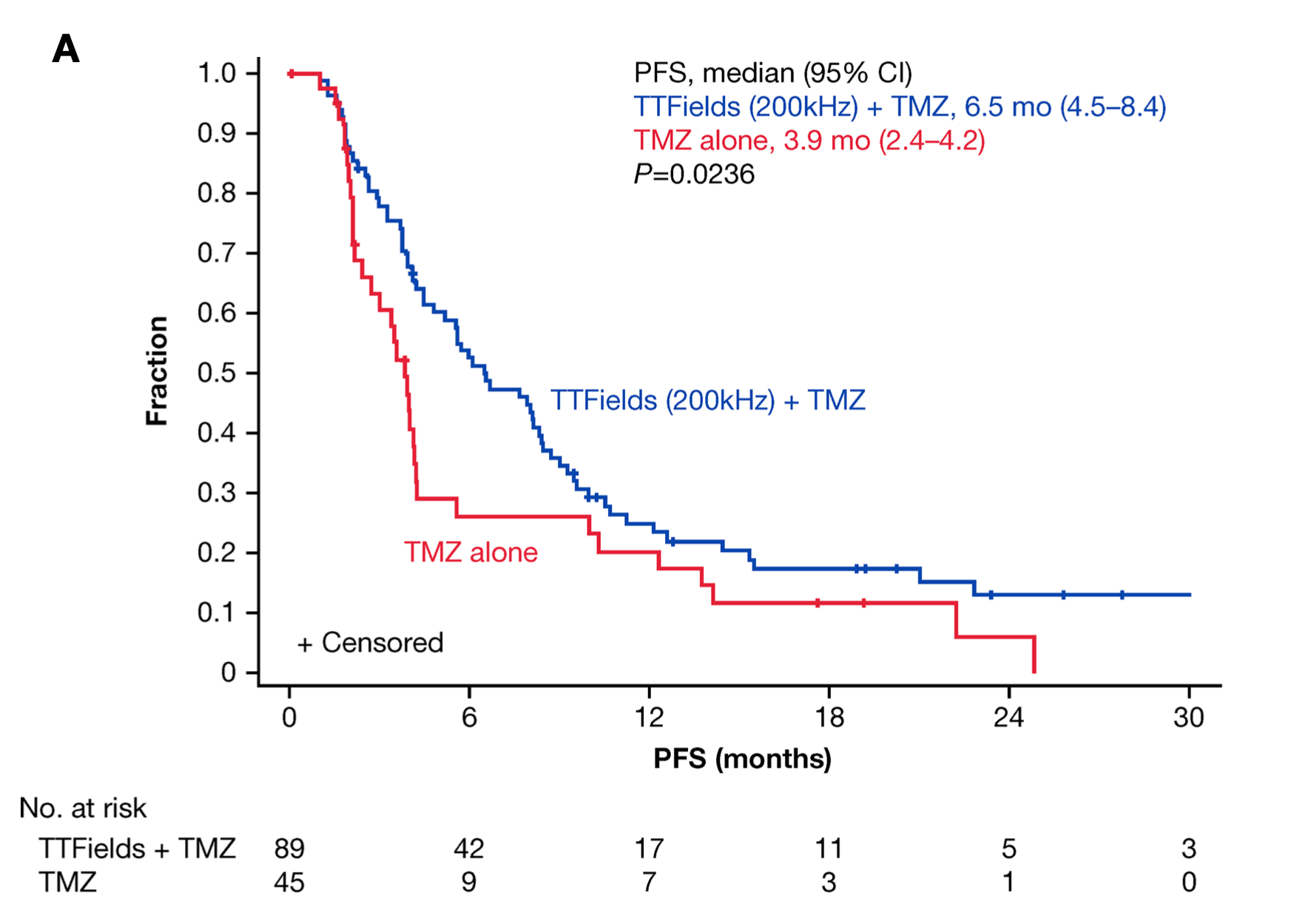
Median duration to follow-up was 8 months for TTFields plus TMZ group vs 7 months for TMZ alone group. Median number of TMZ cycles until first disease progression was 6 cycles and 5.5 cycles for patients in TTFields plus TMZ group and TMZ alone group, respectively. Median duration of TTFields treatment was 7.9 months. CI, confidence interval; OS, overall survival; PFS, progression-free survival; TMZ, temozolomide; TTFields, tumor-treating fields. Adapted from Ram Z, et al. Front Oncol. 2021.
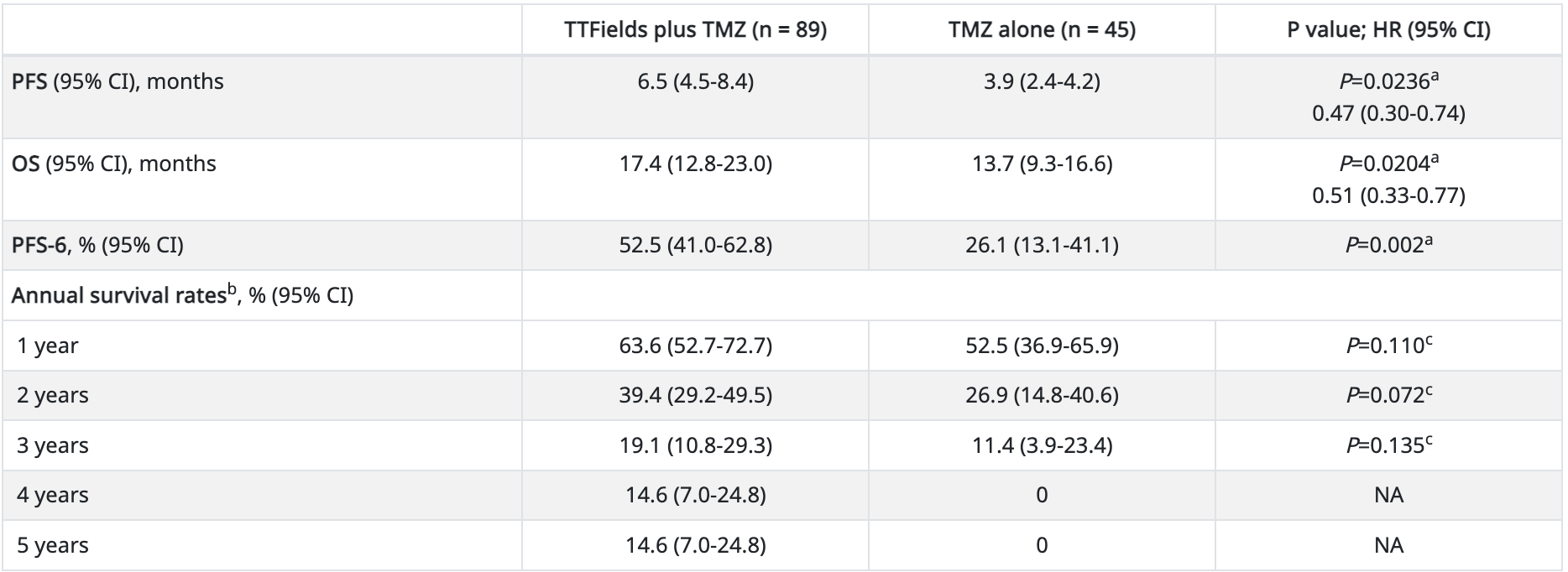
| TTFields plus TMZ (n = 89) | TMZ alone (n = 45) | P value; HR (95% CI) | |
|---|---|---|---|
| PFS (95% CI), months | 6.5 (4.5-8.4) | 3.9 (2.4-4.2) | P=0.0236a 0.47 (0.30-0.74) |
| OS (95% CI), months | 17.4 (12.8-23.0) | 13.7 (9.3-16.6) | P=0.0204a 0.51 (0.33-0.77) |
| PFS-6, % (95% CI) | 52.5 (41.0-62.8) | 26.1 (13.1-41.1) | P=0.002a |
| Annual survival ratesb, % (95% CI) | |||
| 1 year | 63.6 (52.7-72.7) | 52.5 (36.9-65.9) | P=0.110c |
| 2 years | 39.4 (29.2-49.5) | 26.9 (14.8-40.6) | P=0.072c |
| 3 years | 19.1 (10.8-29.3) | 11.4 (3.9-23.4) | P=0.135c |
| 4 years | 14.6 (7.0-24.8) | 0 | NA |
| 5 years | 14.6 (7.0-24.8) | 0 | NA |
CI, confidence interval; HR, hazard ratio; NA, not applicable; OS, overall survival; PFS, progression-free survival; PFS-6, progression-free survival rate at 6 months; TMZ, temozolomide; TTFields, Tumor Treating Fields.
Survival rates are actuarial estimates according to the Kaplan–Meier method. Hazard ratios were calculated for only the primary and secondary endpoints.
aLog-rank test.
bAnnual survival rates are given at 1–5 years after randomization.
cOne-sided Z distribution test.
Total percentage sums may not equal 100 or total percent of a patient subpopulation due to rounding to the nearest integer.
Adapted from Ram Z, et al. Front Oncol. 2021.
Elderly patients with ≥75% (≥18 hours/day) TTFields daily usage had a significantly longer OS than those with <75% TTFields daily usage (21.5 months vs 12.5 months, respectively; HR, 0.52; 95% CI, 0.32–0.86; p=0.0076).8 PFS was 7.9 months in elderly patients with ≥75% daily usage vs 5.2 months in those with <75% daily usage, though statistical significance was not reached in this analysis (HR, 0.69; 95% CI, 0.42–1.10; p=0.0708).8
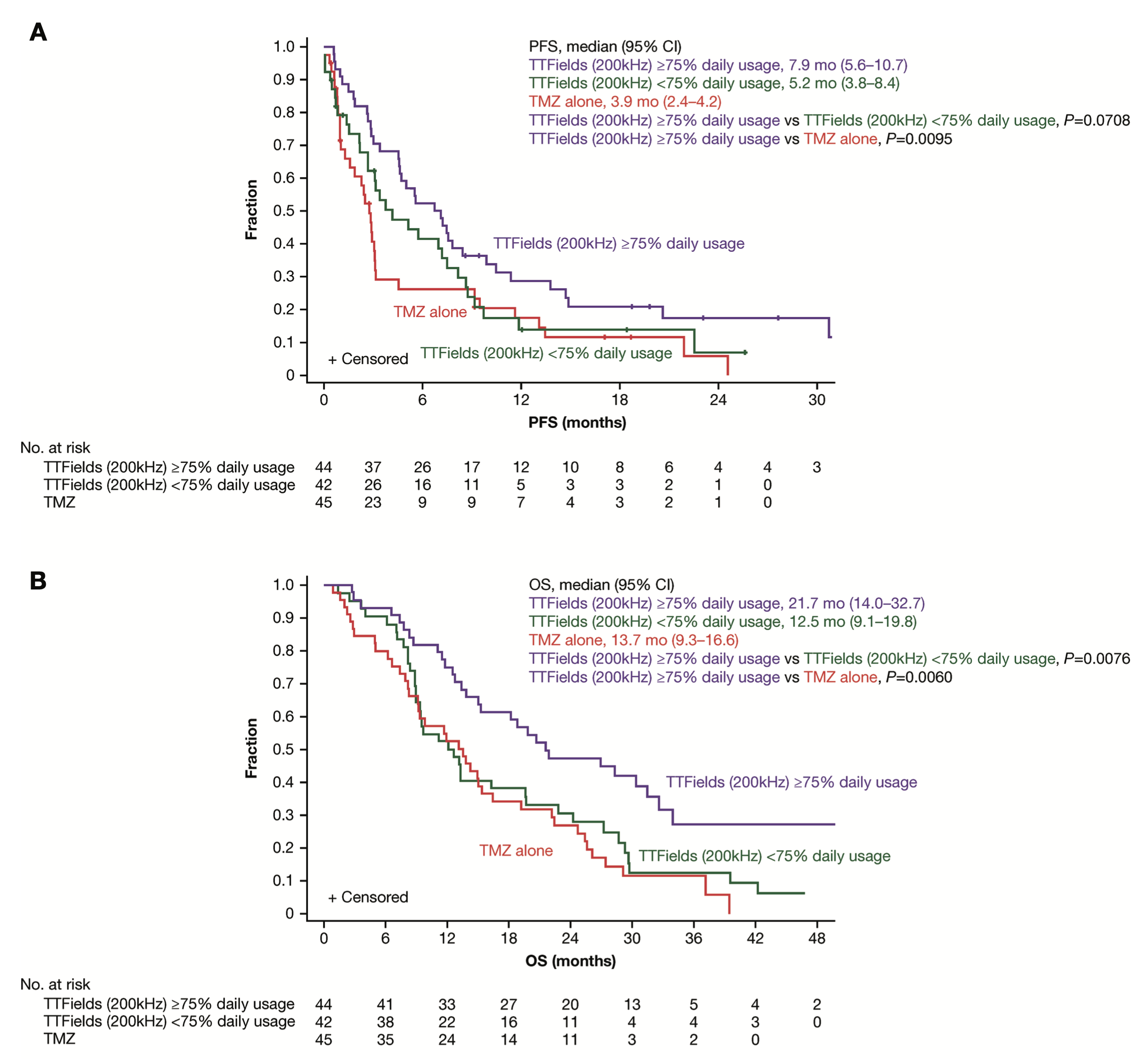
Approximately 57% of elderly patients ≥65 years of age achieved TTFields daily usage of ≥75% (≥18 hours/day). CI, confidence interval; mo, month; OS, overall survival; PFS, progression-free survival; TMZ, temozolomide; TTFields, tumor-treating fields. Adapted from Ram Z, et al. Front Oncol. 2021.
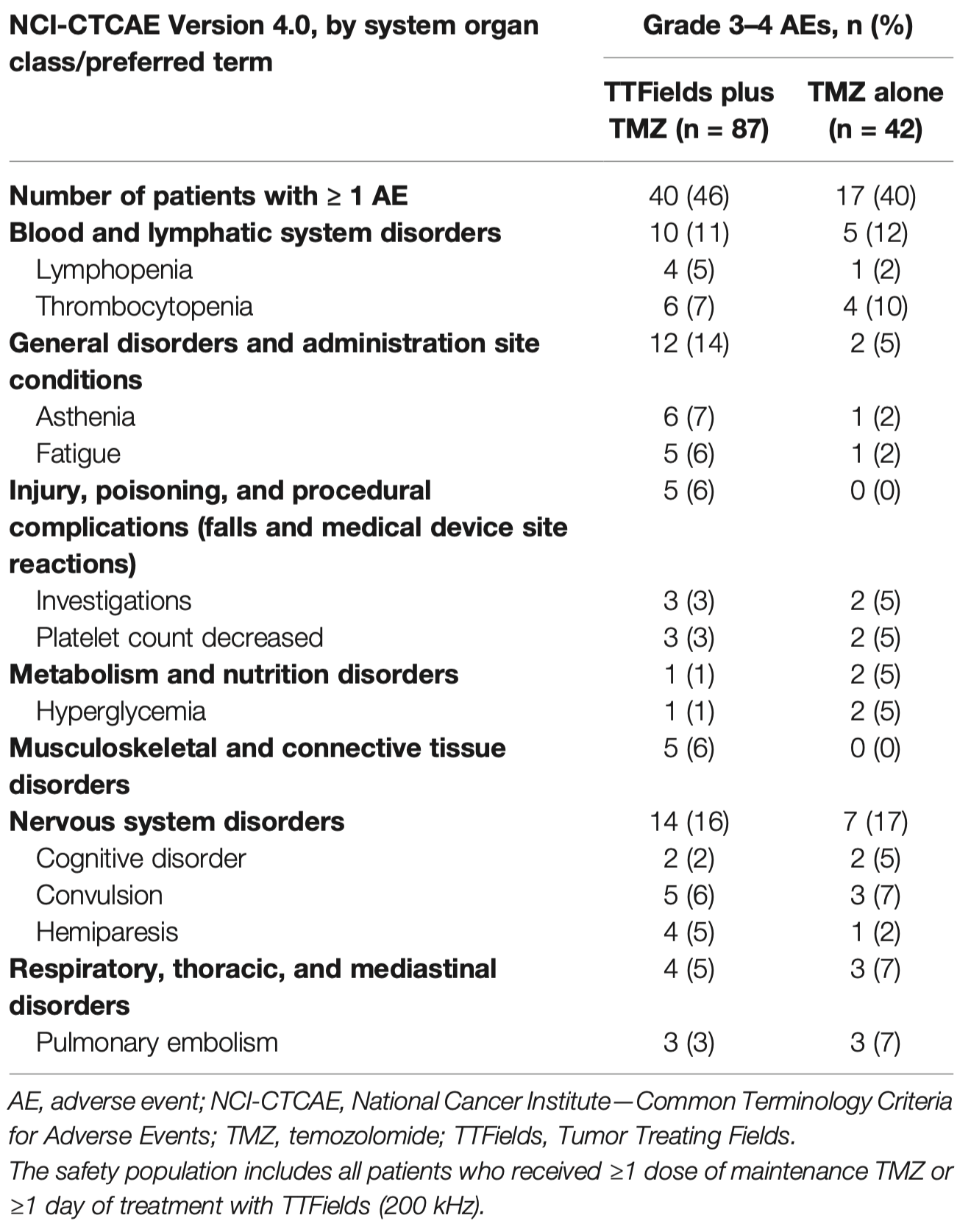
The addition of TTFields to maintenance TMZ in elderly patients was not associated with any differences in the incidence of systemic adverse events (AEs grade ≥3: 46% vs 40%, respectively; p=0.3518).8 Serious AEs (SAEs) were reported by 39% and 33% of elderly patients treated with TTFields plus TMZ and with TMZ alone, respectively.8 No SAEs were reported as related to treatment with TTFields.8
Adapted from Ram Z, et al. Front Oncol. 2021.
As expected, localized skin reactions (medical device site skin reaction beneath the arrays) were reported by 53% of elderly patients treated with TTFields plus TMZ combination.8 Skin reactions beneath the arrays were mild-to moderate (grade 1–2) in 51% of the elderly patients and severe (grade 3) in 2%.8
Impact of treatment with TTFields on elderly patients’ activities of daily life and cognition was analyzed using quality-of-life EORTC QLQ-C30 and QLQ-BN20 questionnaires.2,8 No statistically significant differences in deterioration-free survival (DFS) or time to deterioration (TTD) were observed between treatment groups for any of the preselected items.8
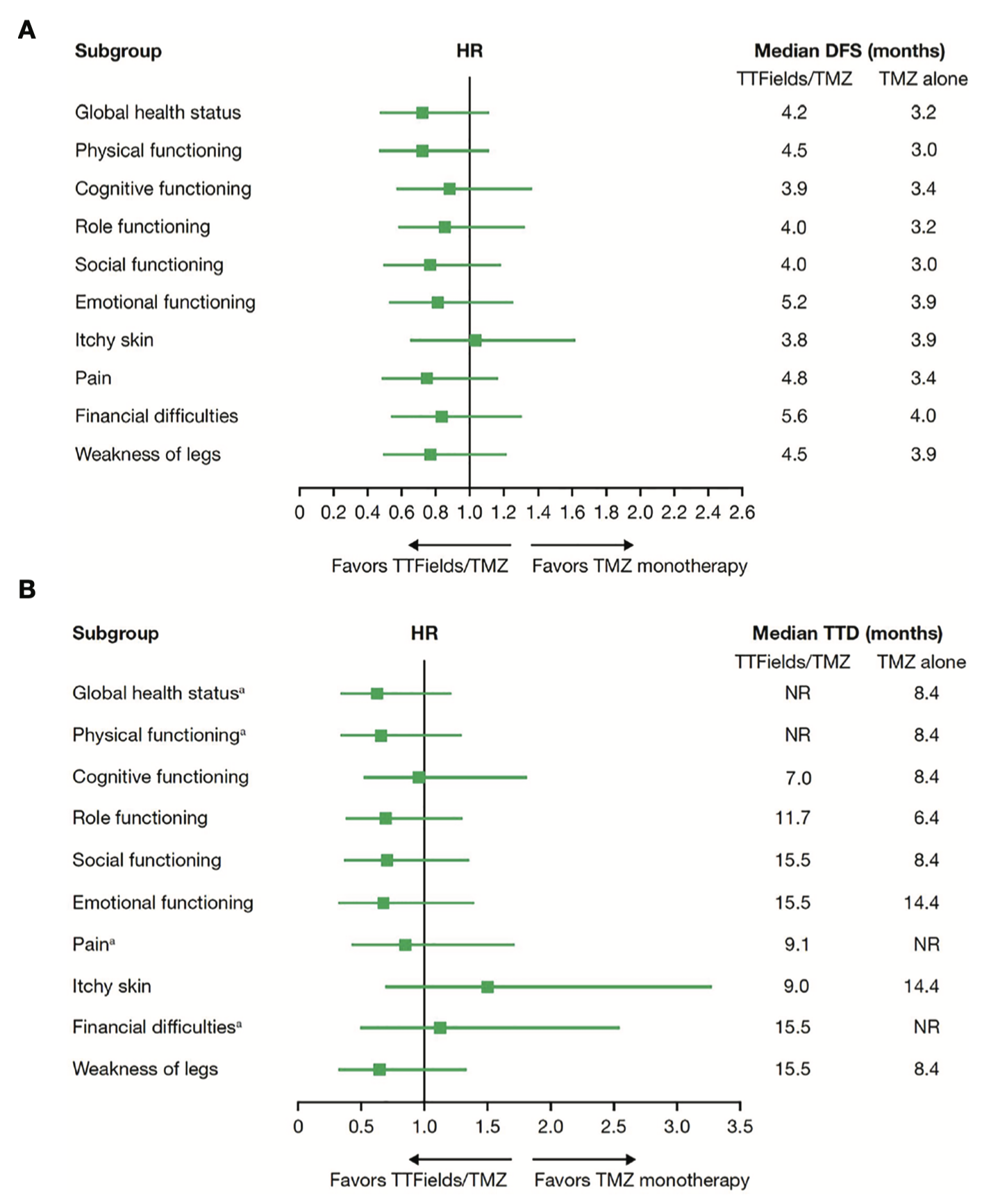
DFS, deterioration-free survival; HR, hazard ratio; NR, not reached; TMZ, temozolomide; TTD, time-to-deterioration; TTFields, tumor-treating fields. aAt the time of this analysis, median TTD was not reached for global health status and physical functioning in TTFields plus TMZ group or pain and financial difficulties in TMZ alone group. Adapted from Ram Z, et al. Front Oncol. 2021.
This EF-14 subgroup analysis suggests that combining TTFields with maintenance TMZ significantly improved PFS and OS in elderly patients ≥65 years of age with newly diagnosed GBM, without significant increases in systemic toxicity or negatively affecting patient HRQoL.8 TTFields-related skin AEs were low-grade and manageable.8
References:
- U.S. Food and Drug Administration approval. Available at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P100034S013. Accessed 6 April 2022.
- Stupp R, et al. JAMA. 2017;318:2306–2316.
- Toms SA, et al. J Neurooncol. 2019;141:467–473.
- Taphoorn MJB, et al. JAMA Oncol. 2018;4:495–504.
- Kesari S, et al. SNO Annual Meeting. 2017. Poster ACTR-55.
- Kim CY, et al. J Neurooncol. 2020;146:399–406.
- Minniti G, et al. Cancers (Basel). 2019;11:336.
- Ram Z, et al. Front Oncol. 2021;11:671972.
EF-11 study in recurrent GBM
EF-11 study was a prospective, international, randomized phase III study designed to compare the efficacy and safety of TTFields monotherapy which was applied at a frequency of 200 kHz to the scalp with investigator’s choice of chemotherapy in patients with recurrent GBM.2 The study recruited 237 patients from 28 institutions in seven countries who were randomized in 1:1 ratio to receive TTFields or chemotherapy as monotherapy.2 Treatments were initiated within 1 week of randomization and were continued until disease progression or intolerance.2
Study design2
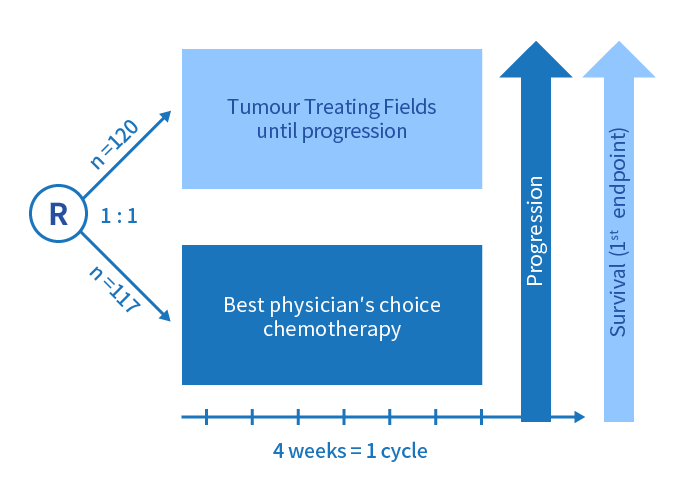
- Primary endpoint: OS
- Secondary endpoints: PFS, percentage of patients alive and PFS at 6 months, 1-year survival rate, radiological response rate, HRQoL and safety
Efficacy
The survival analysis results from the intent-to-treat population are summarized below2:
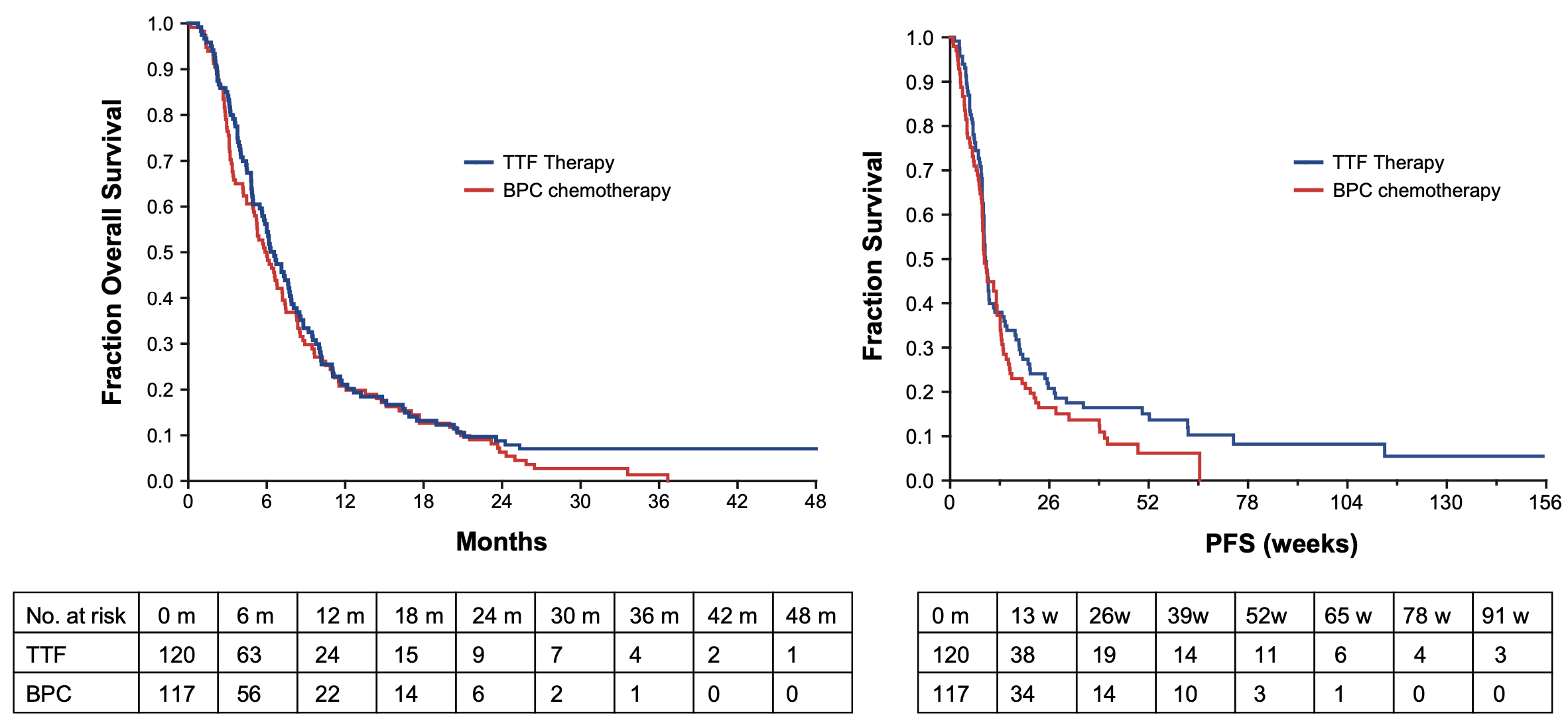
The median follow-up period was 39 months. BPC, best physician’s choice; PFS, progression-free survival; OS, overall survival
| TTFields only (n=120) | Chemotherapy only (n=117) | |
|---|---|---|
| Median OS | 6.6 months | 6.0 months |
| (HR 0.86; 95% CI, 0.66–1.12; p=0.27) | ||
| Median PFS | 2.2 months | 2.1 months |
| (HR 0.81; 95% CI, 0.60–1.09; p=0.16) | ||
CI, confidence interval; HR, hazard ratio; OS, overall survival; PFS, progression-free survival
The efficacy of TTFields appeared comparable to chemotherapy in the intent-to-treat population.2 Numerically more patients achieved partial and complete responses in the TTFields group compared to the chemotherapy group (14.0% vs 9.6%; p=0.19).2
Post hoc analysis on patients receiving at least one treatment course
The mechanism of action of TTFields suggests that the antitumor effect from TTFields requires continuous treatment and disappears when stopped.3 Since the intent-to-treat population of EF-11 study included all randomized patients while 22.5% of patients in TTFields group did not receive a full treatment course of 28 days, it might not be the best population for comparing the efficacy of TTFields against chemotherapy, whose biological effects may persist for 4 to 6 weeks after dosing.3
A post hoc analysis was conducted on a modified intent-to-treat (mITT) population which consisted of 93 patients receiving at least one predefined course of TTFields therapy (28 days) and 117 patients receiving at least one course of chemotherapy.3 This analysis showed that patients in the TTFields group had a significantly longer OS than those in the chemotherapy group (7.8 months vs 6.0 months, respectively; HR, 0.69; 95% CI, 0.52–0.92;χ2 p=0.0093).3
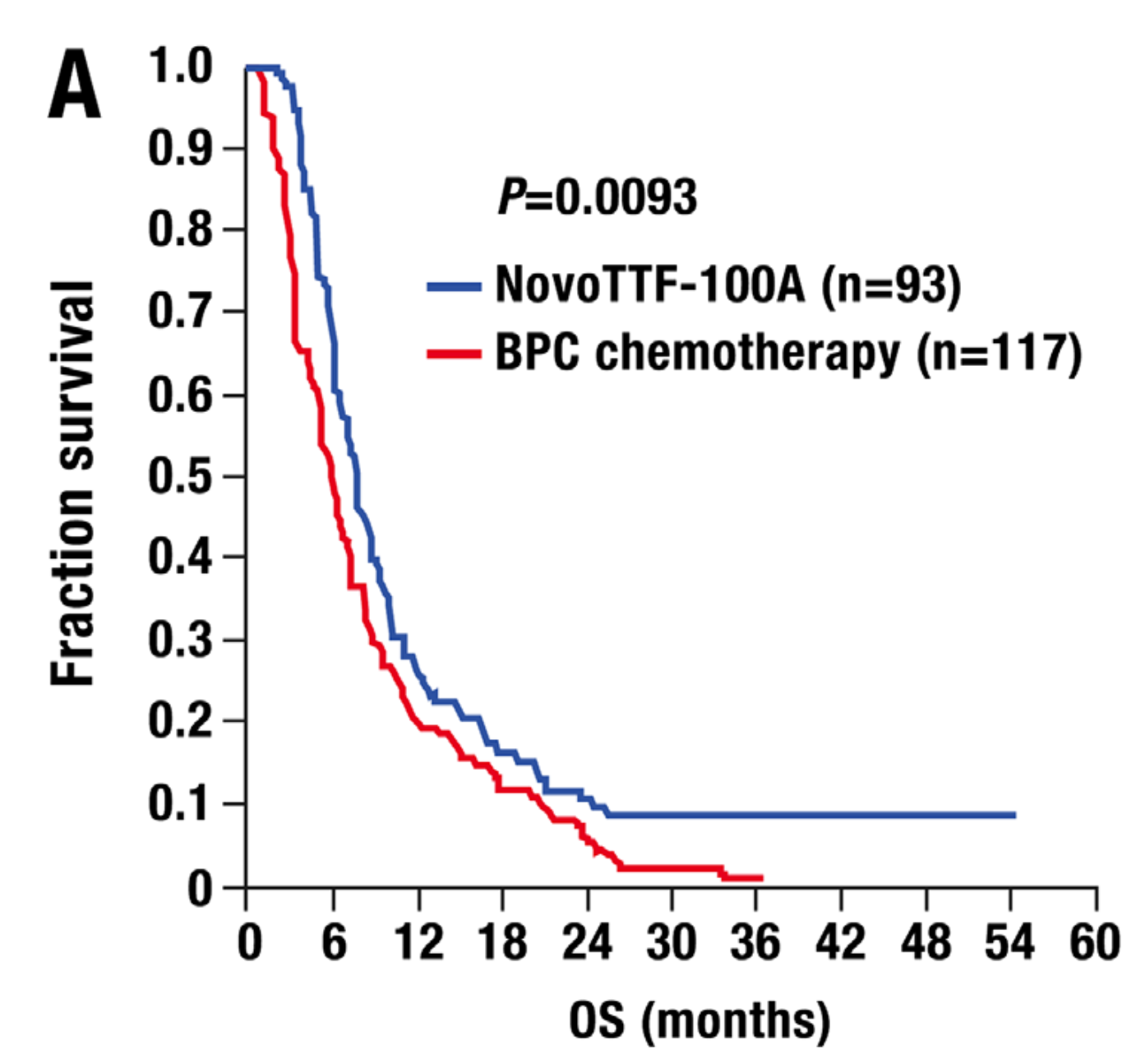
BPC, best physician’s choice; OS, overall survival
Safety
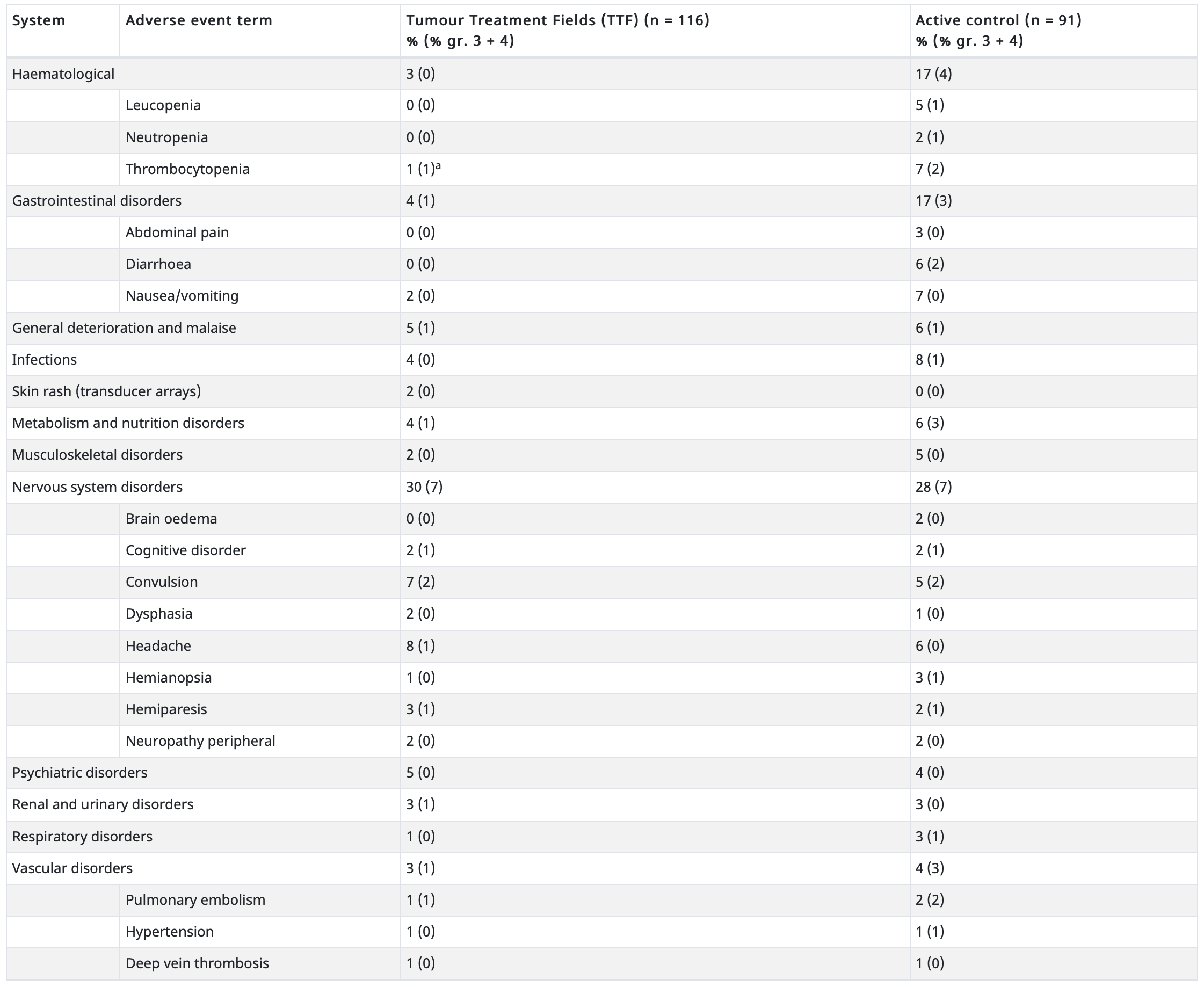
Fewer patients in the TTFields plus chemotherapy group experienced serious adverse events compared with those receiving only chemotherapy (16% vs 6%; p=0.022).2A list of grade 2–4 adverse events by organ system that were seen in more than 2% of patients in either group is summarized below2:
| System | Adverse event term |
Tumour Treatment Fields (TTF) (n = 116) % (% gr. 3 + 4) |
Active control (n = 91) % (% gr. 3 + 4) |
|---|---|---|---|
| Haematological | 3 (0) | 17 (4) | |
| Leucopenia | 0 (0) | 5 (1) | |
| Neutropenia | 0 (0) | 2 (1) | |
| Thrombocytopenia | 1 (1)a | 7 (2) | |
| Gastrointestinal disorders | 4 (1) | 17 (3) | |
| Abdominal pain | 0 (0) | 3 (0) | |
| Diarrhoea | 0 (0) | 6 (2) | |
| Nausea/vomiting | 2 (0) | 7 (0) | |
| General deterioration and malaise | 5 (1) | 6 (1) | |
| Infections | 4 (0) | 8 (1) | |
| Skin rash (transducer arrays) | 2 (0) | 0 (0) | |
| Metabolism and nutrition disorders | 4 (1) | 6 (3) | |
| Musculoskeletal disorders | 2 (0) | 5 (0) | |
| Nervous system disorders | 30 (7) | 28 (7) | |
| Brain oedema | 0 (0) | 2 (0) | |
| Cognitive disorder | 2 (1) | 2 (1) | |
| Convulsion | 7 (2) | 5 (2) | |
| Dysphasia | 2 (0) | 1 (0) | |
| Headache | 8 (1) | 6 (0) | |
| Hemianopsia | 1 (0) | 3 (1) | |
| Hemiparesis | 3 (1) | 2 (1) | |
| Neuropathy peripheral | 2 (0) | 2 (0) | |
| Psychiatric disorders | 5 (0) | 4 (0) | |
| Renal and urinary disorders | 3 (1) | 3 (0) | |
| Respiratory disorders | 1 (0) | 3 (1) | |
| Vascular disorders | 3 (1) | 4 (3) | |
| Pulmonary embolism | 1 (1) | 2 (2) | |
| Hypertension | 1 (0) | 1 (1) | |
| Deep vein thrombosis | 1 (0) | 1 (0) | |
a Thrombocytopenia from prior chemotherapy, normalised subsequently.
Typical systemic adverse events of chemotherapies were not observed in TTFields group while significantly more gastrointestinal, haematological and infectious adverse events were seen in chemotherapy group.2 However, 16% of patients treated with TTFields experienced mild (14%) to moderate (2%) contact dermatitis on the scalp underneath the transducer arrays. This condition was resolved completely after treating with topical corticosteroids.2
Compliance
The median compliance of patients who were randomized to receive TTFields was 86% in each treatment month, translating into a mean use of 20.6 hours/day.2 Post hoc analysis found that patients who achieved a maximum monthly compliance rate of 75% or more (18 hours or more daily) had longer median OS than those who did not (7.7 vs 4.5 months; p=0.042).3 Median OS also appeared to increase in a stepwise fashion with increasing compliance, from 5.8 months with low compliance (<60%) to 6.0 months with medium compliance (60%-79%) and 7.7 months with high compliance (80%-99%) (log-rank test for trend, χ2 p=0.038).3
Health-related quality of life (HRQoL)
Comparing with patients who were randomized to receive chemotherapy, those receiving TTFields reported improvements in HRQoL measured by EORTC QLQ C30.2 Cognitive, emotional and role functioning were found to favour the TTFields arm.2 No significant difference in global health and social functioning was observed between the two arms.2 The improvements in HRQoL were likely driven by the statistically lower incidence of serious adverse events experienced in the TTFields arm compared with the chemotherapy arm.2
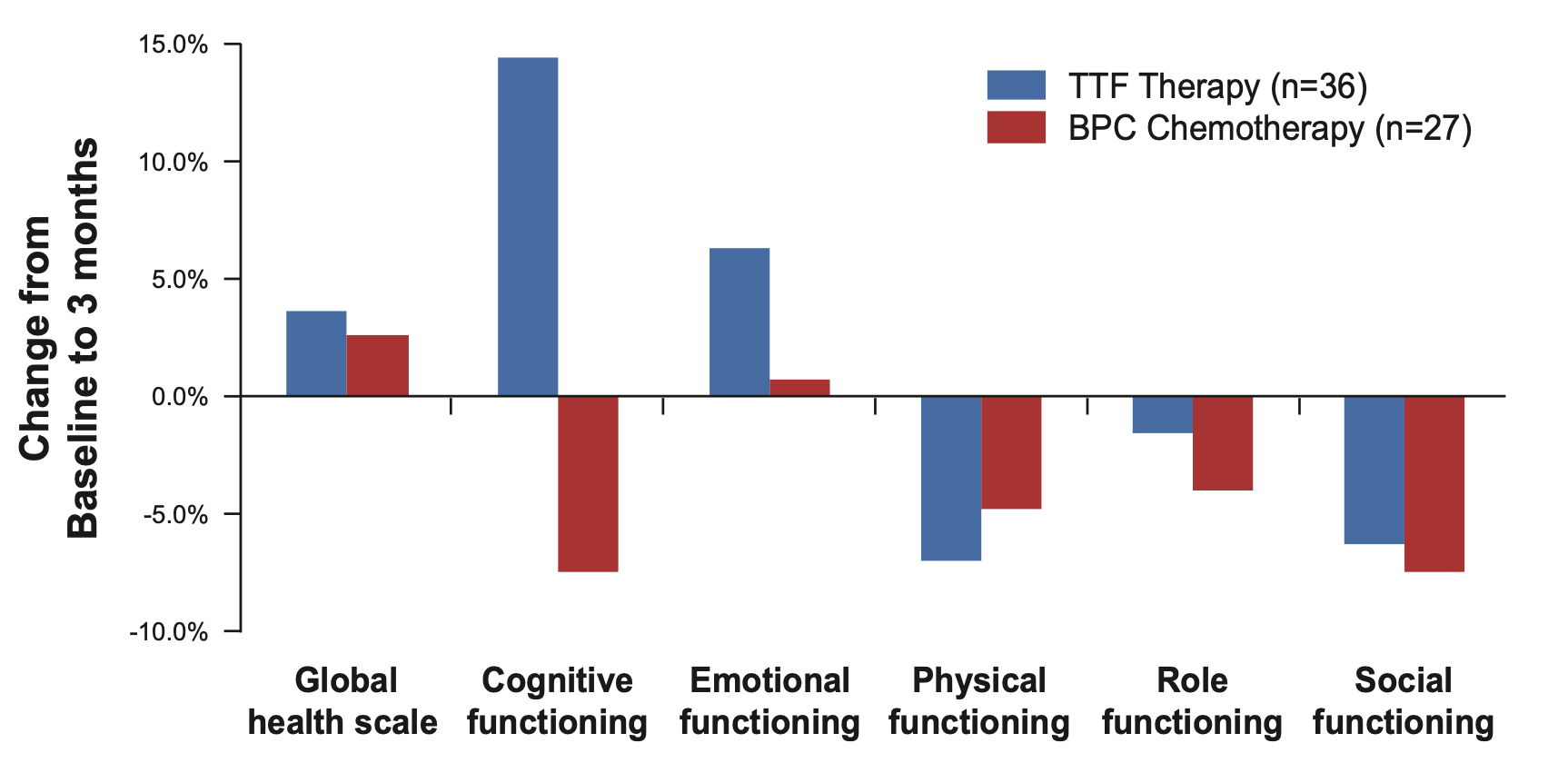
BPC, best physician’s choice
References:
- U.S. Food and Drug Administration approval. Available at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P100034S013. Accessed 6 April 2022.
- Stupp R, et al. Eur J Cancer 2012;48:2192–2202.
- Kanner AA, et al. Semin Oncol. 2014 Oct;41 Suppl 6:S25-34.